A common occupational hazard for physicians is the late night call from a frantic friend asking about a worrisome medical issue. I get my fair share of questions pertaining to symptom management, terminal illness, hospice and death, which I am more than happy to help with. Occasionally, however, I get questions about kids. As an internist and a palliative care physician, nothing sends chills down my spine like a question about kids. Fortunately for me (and my group of friends) we have a pediatrician among us. So when I get that call asking about a rash, a fever, a head bonk on the playground or weird looking poop, I can simply say “Ask Jenna!”
I met Dr. Jenna Miller over 20 years ago when we were both undergrads (pause for mid-life crisis freak out moment). She was a couple of years ahead of me in medical school and helped me navigate my way through the first two years of hard core foundational lectures and then the final two years of clinical rotations. She went on to specialize in pediatric medicine and then completed a 3 year fellowship in pediatric critical care. She is the doctor who takes care of the sickest of the sick kids…kids who are so sick that they wind up in the pediatric intensive care unit. She is probably someone you never want your kids to have a reason to meet, but if your kid is that sick, she is undoubtedly the person you want taking care of them.
She and I have been in close contact since the beginning of the Covid pandemic, sharing notes and experiences. Though our scope of practice could not be more different, our fears, worries, frustrations and heartaches are very much the same.
With the ever changing Covid landscape and the emergence of the Delta Variant, there has been a lot of conflicting information circulating in the news and on social media. We hear of hospitals in Texas and Florida that are overflowing and having to ship sick kids out of state, but then we hear about local county dashboards where covid numbers appear to be much lower.
So with all of this confusing information floating around, I did what I always do…”Ask Jenna!”
Despite being elbow deep in an insanely busy pediatric ICU, she was gracious enough to answer several questions for my blog. You will find that her answers are not only incredibly thoughtful, they are rooted in evidence and data as well as her own first hand experience. I hope that you will find the following information helpful as we all continue to navigate this pandemic.
So…a lot of people out there have heard that Covid doesn’t really affect children. What would you say to them?
Covid has always affected children since the beginning of this pandemic. Data was published last year in the Journal of American Medical Association that children with chronic medical conditions acquired acute covid and more recent literature discusses healthy children acquiring the post covid inflammatory process called MIS-C, or Multisystem Inflammatory Syndrome in Children. Acute covid mostly affects the respiratory system while the post covid MIS-C process can affect multiple systems and both can lead to ICU admissions for heart or lung failure. There is also an entity called MIS-N which affects newborns and we are still very early in our understanding of this. Neonates (newborns) in our city have this right now.
Currently, we have a higher percentage of total cases affecting children nationally. I have seen numbers ranging from 1% previously to 15% now as reported by the American Association of Pediatrics. There are also higher numbers of children overall requiring hospital admission, including healthy children. 391 children have reportedly died from the disease thus far nationally. On Aug 9 a report published by the CDC stated that 94,000 cases of pediatric covid had been diagnosed the previous week with an average of over 200 children hospitalized per day. Covkidproject.org tracks hospitalizations by age and state and is one of the only current resources we have for this information. Of note, Children’s mercy diagnosed over 200 children with covid in a recent week where data is available.
In addition to being affected by the virus, are kids also spreading it?
Early on we saw children had lower rates of reported infections. According to the CDC, this could be that children’s activities (school, sports, daycare) were mostly shut down and children were less likely to be tested. However, in some surveillance screening children and especially teens sometimes showed a higher rate of infection while still having minimal symptoms. The community viral burden has been shown to be fairly well correlated with school transmission thus if community COVID19 viral burden is high, the introduction into schools is much more likely. Similarly, staff to student and student to student transmission rates seem fairly low by studies suggesting students and staff are acquiring it outside of schools, in the community thus far. We have however not pressure tested these findings by sending kids back to school en masse during a national surge.
Are you seeing an increase in Covid-19 in kids in the ICU?
We have had a higher census with both acute covid as well as viruses we usually see in the winter such as RSV and rhinovirus/enterovirus. We saw that in Australia and Brazil during their summer months this past year and we are seeing it now. This is in addition to the usual summer trauma and surgical patients. We do have more acute covid now in the ICU than during any other time during the pandemic.
The surge has once again changed what PPE we need to wear in the hospital and how we can interact with each other and our patients. By this I mean, we must remain masked at all times except while eating.
How have Covid infections in kids changed with the emergence of the Delta Variant?
This graph is the latest from the CDC regarding new admissions of children to the hospital. We are at a higher rate per 100,000 children than ever before during the pandemic. The data reported by the CDC shows states with the highest pediatric admissions rates are also the ones that have banned mask mandates in their schools. We don’t yet have enough US data to state with certainty if Delta is making children sicker or if we just have more of it in the community.
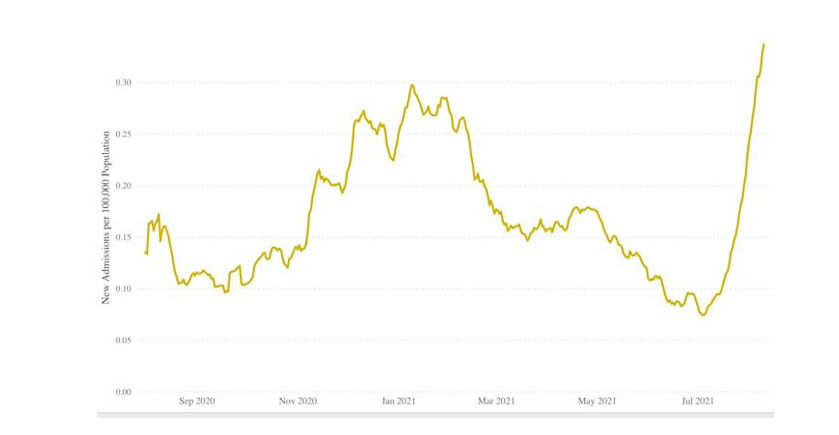
The most granular data we have can be found at covkidproject.org with state by state case, hospital admission and mortality rates.
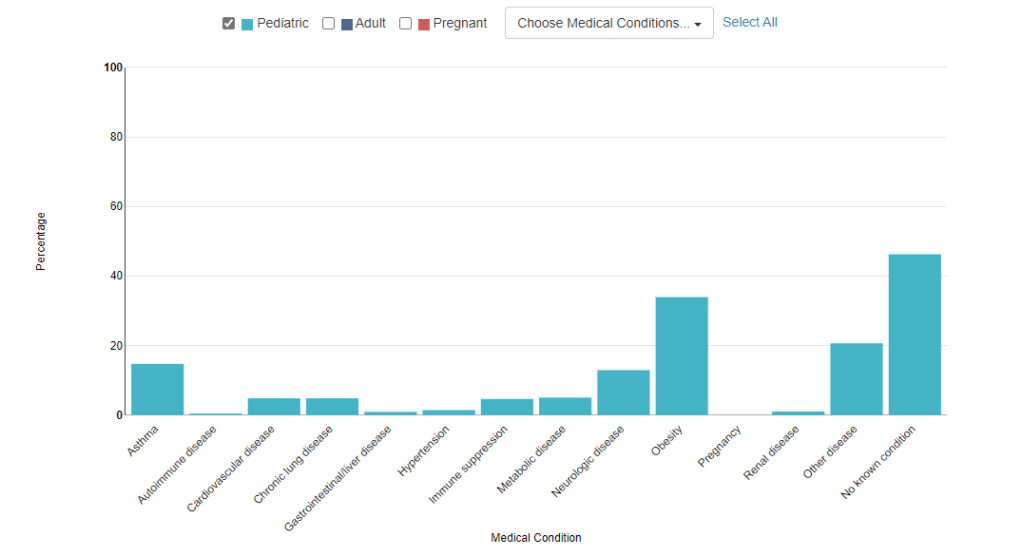
Are the kids you are taking care of with Covid generally healthy or do they have underlying health issues…or both?
The answer is both. Previous data says that most acute covid pediatric patients had underlying health issues such as prematurity, asthma or chronic lung disease. This continues, however we are seeing acute covid in healthy children now complicated by pulmonary embolisms, or clots in the lungs. Recent data listed below is consistent with my anecdotal experience.
Where do kids seem to be getting Covid? (friends, un-vaxxed family, camps, sports…?)
Anecdotally, Many have gotten it from inside their own homes with unvaccinated family members
What are the best ways that we can limit transmission of Covid in kids?
We know the tools for limiting transmission. Masking inside, avoiding large groups and vaccination for those 12 and up now. Additionally, with only 45% of Kansas and 42% of Missouri being fully vaccinated, adults getting vaccinated can help our children too by limiting community spread. Unchecked spread has led to the current variants we are seeing. Viruses are “smart” and will continue to mutate until we don’t allow future hosts to contract the disease. Of note, 95-98% of those admitted to the hospital are unvaccinated. Some individual hospital data shows that 100% of those in the ICU and on ventilators are unvaccinated.
Another point here is frequent testing. Families should test often for ANY cold symptom, even if mild. Over the counter testing is now available. If there is an in home positive, isolation of that family member, as much as possible, should be attempted. This includes using separate bedrooms and bathrooms and masking in your own home.
Link to at home covid test kit.
As a critical care doctor who knows a lot about respiratory mechanics and blood gasses, do you have any concerns about kids wearing masks during the school day? Will they have lower oxygen levels, higher CO2 or be at risk of other infections from dirty masks?
Surgeons, anesthesiologists and other medical personnel have long worn masks all day for patient care activities. There are great observational reports that wearing a mask does not affect your oxygenation levels while on medical monitoring. As for carbon Dioxide, the size of this particle is 0.33 nanometers. The size of our respiratory droplets, which house covid, are 20-2000 micrometers. There is no surgical or cloth facemask which will hold carbon dioxide in. Notice that the measurements aren’t even the same. A nanometer is 1000x smaller than a micrometer.
Any dirty surface can potentially have what we call fomites on them. Fomites are objects that can have active infectious particles and transfer them to a human host. This can be said for one’s shirt, shoes or lunchbox. A mask is just an additional piece of one’s apparel these days and should be washed as our clothes are washed.
Here is a link to a site about masks and children sponsored by the American Academy of Pediatrics.
There is also a lot of concern about vaccine safety. Do you think that the vaccine is safe, and would you recommend it?
The vaccine is safe. I have been vaccinated for 8 months and have no side effects. I recommend it to anyone who does not have a history of vaccine reactions in the past. It does not alter your DNA and the RNA actually degrades rapidly leaving only the affect of training our immune systems to recognize and fight COVID.
It was developed more rapidly than previous vaccines which people question. The process usually takes years to achieve. However, as there were more financial resources available as well as no shortage of volunteers, the process went quickly. Manufacturing was also begun before approval which also is atypical due to financial burdens. This is what we can do with unlimited financial and human resources in research.
Have you seen any kids in the hospital due to side effects from the vaccine?
We had one suspected post vaccine case of myocarditis who recovered quickly. However, the overall incidence of this disease process is higher in covid patients than in those receiving the vaccine. And the number of cases and admissions we prevent with the vaccine far outweighs this risk. I’ll add there is zero data suggesting decreased fertility for vaccinated individuals which I hear pop up frequently and I also have zero understanding of where this concern came from.
What activities are safe for kids to participate in right now and what would you advise against?
Outdoor activities are ok. Sports that do not allow for physical distancing have higher rates of transmission as do any activities that require singing/heavy breathing indoors.
Small indoor groups with vaccinated individuals are ok. I would avoid large indoor groups with unknown or unvaccinated groups. I would mask with anyone not in your family unit when indoors, outside your own home.
How is morale among health care workers taking care of kids right now?
Health care workers in general are tired. There was no break for us last year and the work was, in fact, harder with an unknown disease, new treatment strategies to learn, ever changing PPE requirements and possibility and fear of transmission to our families. There was but only a small break this spring before the summer surge started and now we are busier than any other time in the pandemic. We are tired and need help to slow this surge down.
Any final thoughts?
With school beginning around our community, I implore people to vaccinate, mask and frequently wash their hands. If this were the beginning of the pandemic, we would all be appalled at the rate of rise of infection in our children and of hospitalizations. Most children will be fine when affected with COVID, however even in that best case scenario, they can still be a vector of transmission to other children and adults who will not be fine.
And lastly, the mental health of our community’s children is also in crisis. Our very own Dr. Jensen who is the chief health advisor for Blue Valley School District, recently published a book about helping students during and after the pandemic called “After the Mask: A guide to caring for students and schools.” This is a great resource to help support mental health for our youth.
Above all, let’s take care of each other. Our ability for compassion and connectedness is what makes us human.

This is the kind of information that many parents & grandparents are searching for. Thank you! We must protect our kids; above all else.
LikeLike