Death certificates…ahem.
I love Sunday mornings. Things move at a slower pace. Danny and I enjoy coffee together on the deck. The kids generally sleep in a bit and eventually roll out of bed to help me make cinnamon rolls before we watch church online. So when my alarm clock went off this morning, I opened my eyes with all of the hope and expectation someone suffering from chronic rage could possibly expect. It lasted about 5 minutes.
Today, social media is being plastered with the most absurd misinterpretation of data that I have ever seen. Until tomorrow, I’m sure.
The following snippet from the CDC’s website caused the conspiracy theorists to lose their collective minds and gave them, what they thought was, ammunition to dispute the actual death toll of Covid-19 (you can find the page here):
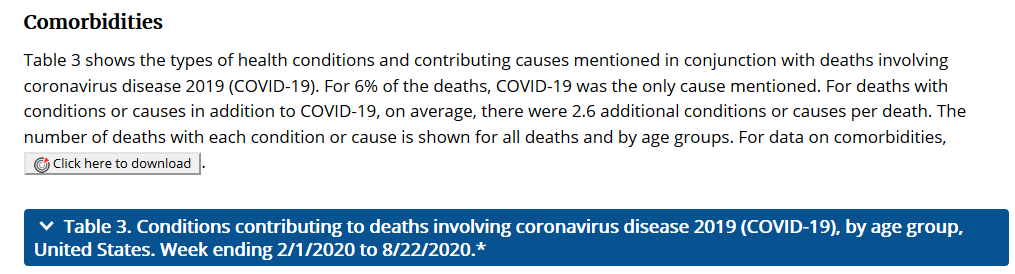
I understand that not everyone is familiar with how death certificates work, so I present to you: Death Certificates 101, and why “For 6% of the deaths, COVID-19 was the only cause mentioned” means absolutely, freaking, zilch, zero, nothing.
So…for a little background. I am a Hospice and Palliative Care doctor. I have completed hundreds of death certificates, and thus, am familiar with how all of this jazz works. I’ll be the first to tell you when I am out of my wheelhouse, but this my friends, IS MY WHEELHOUSE!
Death certificates capture a person’s cause of death and the events or conditions leading to this event. Below is a generic version of a blank death certificate.
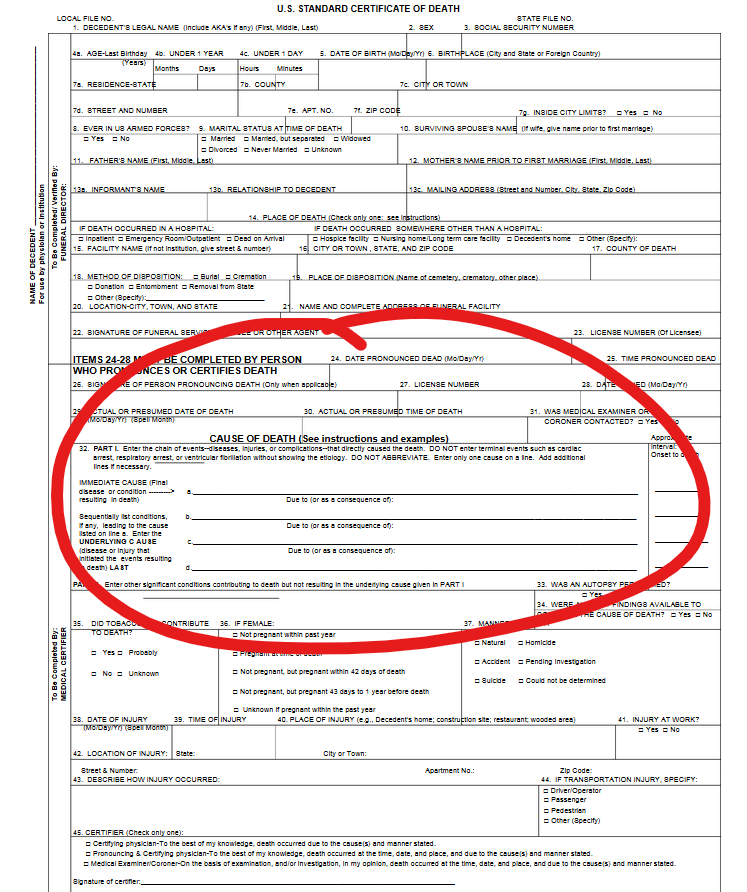
Within the red circle is where the physician documents the immediate cause of death (top line) and then lists the conditions that contributed to the immediate cause of death (next three lines).
I don’t love filling out death certificates because the chain of events isn’t always easy to tease out. Sometimes an elderly person just stops eating and dies under the care of hospice, but I don’t have any labs or imaging to inform my determination of what exactly they died from. Was it renal failure from dehydration or was it an aspiration event that lead to pneumonia? I don’t love listing an immediate cause of death as “stopped eating…?” And a contributing condition as “old…?” I prefer that my death certificates make good sense and be wrapped up in a tidy little bow.
My favorite (okay, weird choice of words, but hang with me) cause of death to document is ischemic cardiomyopathy (heart failure due to coronary artery disease). The chain of events are usually very clear cut and occur in a step wise fashion that I can easily document. A death certificate from ischemic cardiomyopathy would probably look something like this:
Immediate cause of death: Hypoxemic Respiratory Failure (from fluid building up in the lungs)
Due to: Chronic Systolic Heart Failure
Due to: Coronary Artery Disease
Now if this person had other conditions that contributed to their death, I would list these in the box for “Other significant conditions contributing to death, but not resulting in the underlying cause given in Part I.” In the above scenario, these might be things like hyperlipidemia (cholesterol), chronic kidney disease, hypertension, atrial fibrillation.
So, now…with that background information, let’s talk about Covid-19 and how a physician (such as myself) might go about completing a death certificate when Covid-19 is the cause of death.
We all know that Covid-19 is a respiratory illness and primarily causes death by leading to things like ARDS (acute respiratory distress syndrome), pneumonia, septic shock, renal failure and thrombotic events like strokes. Let’s take for example a hypothetical patient, John. John is 62 and has mild hypertension (like a fair amount of 62 year olds do) and is a little bit overweight (again…62 year old man). He works full time at Lowe’s and enjoys hanging out with his grandkids on the weekend. He contracts Covid-19 from his youngest son who came to visit from Florida. He is admitted to the hospital and develops worsening respiratory failure which is due to ongoing Covid-19 infection and related inflammation. He is intubated due to very low oxygen levels and work up demonstrates that he has ARDS. His body continues to deteriorate and he develops shock (low blood pressure requiring vasoactive medications to keep him alive) and acute renal failure requiring dialysis. He eventually dies.
The next day, you receive an email from the state notifying you that his death certificate is ready to be completed.
What should we choose as the immediate cause of death?
I would go with”Hypoxemic Respiratory Failure.”
Okay, moving on to line 2. What lead to John’s Hypoxemic Respiratory Failure?
It seems that ARDS was the condition directly leading to the Hypoxemic Respiratory Failure. So I would type “Acute Respiratory Distress Syndrome” into line 2 (the freaking death registry doesn’t like it when we use acronyms…grr).
Now line 3…what lead to John’s ARDS?
This is where we would list Sars-CoV-2.
Strong work so far, friends!
Now on to the box for other conditions that may have contributed to death, but weren’t directly related to the underlying cause, which in John’s case was Sars-CoV-2.
It would probably be reasonable to list “Hypertension” and “elevated BMI” as conditions that may have contributed to death as we know that hypertension and obesity are risk factors for death in Covid-19.
Now sign your electronic signature, hit CERTIFY and it’s off to the state!
Lets look back….
We have listed “Hypoxemic Respiratory Failure,” “ARDS,” “Sars-CoV-2,” Hypertension” and “Elevated BMI” on John’s death certificate. If you are counting, those are two acute conditions (respiratory failure and ARDS) and two chronic conditions (hypertension and elevated BMI) not including Covid-19. You can see how the list of diagnoses can lengthen…. We didn’t even mention “shock” and “renal failure.”
Lets consider a different scenario. Jennifer is 35 and perfectly healthy. She is a waitress at a restaurant and probably contracted Covid-19 from a large, indoor table of loud individuals, several of whom were coughing. She comes to the hospital because she is having a hard time breathing. She immediately decompensates in the Emergency Room and is intubated. A CT scan shows multifocal pneumonia and a small pulmonary embolism. She is started on broad spectrum antibiotics and anticoagulation. Her test for Covid-19 comes back positive and she is taken to the intensive care unit where her oxygen levels continue to fall and her heart stops beating. Despite CPR and chemical interventions to resuscitate her, Jennifer dies.
Her death certificate is routed to you the following day. Here we go…
Immediate cause of death: We could go with “Hypoxemic Respiratory Failure” again for Jennifer.
What lead to this? I would list “Multifocal Pneumonia” though you could make a case for the pulmonary embolism as well.
And what caused the Multifocal Pneumonia? This is where we list Sars-CoV-2.
Other contributing conditions? Jennifer doesn’t really have any – we can leave that box empty.
So even in this otherwise healthy 35 year old woman, her death certificate will list Sars-CoV-2 as well as two other diagnoses.
Lordy…is anyone even still with me here? If you are (and props to you, by the way), you’ve probably figured out that a death certificate with ONLY the diagnosis of Sars-CoV-2 doesn’t even make sense. Jennifer didn’t go from perfectly healthy to dead from Covid-19 without SOMETHING HAPPENING in the interim. When people die from Covid-19, they die because the virus has caused something to go very wrong in their body. I would go so far as to argue that the doctors completing the death certificates on those 6% without any other factors listed were either 1) in a hurry, 2) lazy or 3) didn’t understand how to fill out a death certificate in the first place. I would be embarrassed to submit such a half-assed death certificate, personally!
If you look at Chart #3 from the CDC (here’s the link again – you’re welcome), you will see that the conditions listed are a mishmash of both chronic and acute illnesses. Things like ARDS, pneumonia, respiratory arrest and cardiac arrest are all acute illnesses most likely CAUSED by Covid-19. Other conditions like chronic lower respiratory disease, hypertension, diabetes and Alzheimer’s are all more chronic conditions that could have been exacerbated by Covid-19 or predisposed to a poor outcome. I’ll let you peruse the chart for yourself.
Seriously….you’re still here? You have my permission to stop reading and go grab a drink. This has become way more tedious than I generally prefer, but such is data and science.
One more example before I shut the hell up and get myself a drink. Mike is a 19 year old kid. Totally healthy. He gets shot in the chest walking home one night and is immediately taken to the hospital. Despite heroic efforts by the trauma team, Mike dies. Mike’s death certificate will likely include “hemorrhagic shock” as the immediate cause of death. This was caused by a “traumatic injury to the aorta” which was the direct result of a gunshot wound. Does the fact that the gunshot wound caused hemorrhagic shock mean that Mike didn’t die of a gunshot wound?
Okay, I’m really done. Thanks for hanging in there with me. I didn’t have my editorial team (Danny) proofread this one because he is out picking up dinner. And because this seems to be an incredibly hot topic today and I wanted to get this out ASAP.
Feel free to leave comments if you have questions or feedback. This is something that needs to be clearly understood.
Much love,
Dr. B

This is an awesome blog post. Thank you so much for clearing the air so to speak. I have not been posting things on my FB page because I am so tired of people, many of who do not even know me, Juno all over me because my beliefs are different than theirs but I may post this just because it is so important to me. Thank you again.
LikeLiked by 1 person
Thank you so much, Dr. Bartlett for going through all that. I’m going to post it on social media so there is more information out there-I feel sure you’d be ok with that!
LikeLiked by 1 person
Thank you for this clear response from your wheelhouse! I am a family physician, but since I only see outpatients in my office, it has been many years since I completed and signed a death certificate. It is great to have a definitive response.
LikeLiked by 1 person
I thank you for this clearly written & well explained post. I am tired of the crazy things that every day people & politicians are saying about false Covid cause of death documentation. As if more than 200,000 people in the U.S. concidentally died with the same symptoms unrelated to Covid in the past 6 months. All reasonable people know that other deaths without documented Covid are likely numerous as well. People who didn’t get tested after fatal heart attacks or strokes, homeless people found without obvious causes of death, etc. But reasonable people are few & far between these days. Also, I so appreciate your sense of humor. Much meeded in this frustrating time.
LikeLike
So you agree that just like the 6% is misrepresented, the 180k deaths is also misrepresented?
Mike, 19, shot in the chest, dies from hemorrhagic shock caused by traumatic injury to the aorta. He tests positive for Covid which he got 11-weeks ago. It is listed as a comorbidity. He is counted in the Covid death count.
LikeLike
James, good question. We already know that death certificates are flawed…either due to user error or incomplete data to rely on to fill out a DC appropriately. I know that there are instances of Covid popping up on death certificates when it clearly shouldn’t have. In the case of Mike, Covid did not contribute to his death in any way, shape or form, so should 100% be left off of the death certificate. Where it gets a little dicey is in the case of people who have heart attacks and strokes and also test positive for Covid. We know that Covid causes significant blood clotting so it would be very appropriate to draw the conclusion that if someone had covid and a heart attack, it was likely related and contributed to their cause of death. I would suspect (though there is no way to know for sure) that there are a significant number of people who have died of Covid-related morbidities who were never tested for Covid, and thus, it does not show up on their death certificate.
LikeLike
I probably should have affirmed this before but I appreciate your commentary on all of this. It was very informative. It’s interesting how the Covid death count has become some sort of barometer for how well (or not) we have done in managing the pandemic. The cause of death is a much more complicated matter. So it seems, rarely does one thing kill you (Covid related or not).
LikeLike
Something I know I have learned is that all data is flawed. So one of the most important steps in data analysis is understanding the sources of bias and collection methodology. Your explanation was amazing. Thank you.
I think a way to describe the data is not to think of it as “deaths caused by COVID-19” but rather “deaths concomitant with COVID-19” which respects that not all deaths were caused by it, but is helpful in coming to an understanding of its concomitance.
LikeLike
Hi Doc. So what do you attribute the 6% death certificates? Is that just laziness on the doctors’ part? Thanks for adding your knowledge to the dialog.
LikeLike
My inclination would be that the doc was in a hurry, lazy, didn’t have the full chart to review before completing the DC, or simply hadn’t been educated on how to appropriately complete a DC.
LikeLike
I’ve heard another doctor list that they were probably lazy, rushed, or depressed/overwhelmed (from the sheer number of covid deaths that they’d dealt with?)
LikeLike
Thanks, you confirmed my own intuition—it’s that 6 percent that interesting.
LikeLike
Hey Dr Bartlett – I first want to say thank you for your COVID series blog posts and thank you for all that you do as a palliative care physician 😊
Your mom and you actually took my senior pictures at SMN waaaaay back when, haha. I graduated from North with your brother-in-law, Joey. I worked at KU after nursing school and remember you were doing your fellowship as I was finishing up my NP program. Fast forward and I’m now actually a palliative care NP at Banner University Medical Center in Phoenix! I’ve loved reading your blog posts because you’ve so perfectly been able to put into words how I’ve felt working in palliative care these last few months.
So thank you again! I look forward to your continued blog posts. Hope you and your entire family are staying healthy and well!
Take care!
Cara
LikeLiked by 1 person
Cara! Great to hear from you. That’s wonderful that you are a PC NP!!! Stay safe in AZ!
LikeLiked by 1 person
Hey Dr. Bartlett! First, I just want to say thank you for sharing your COVID series blog posts with others and for all that you do as a palliative care physician. You and your mom actually took my senior photos at SMN waaaaay back when, haha! (I graduated from North the same year as your brother-in-law, Joey.) I later worked at KU after nursing school and remember you were in your fellowship when I was finishing up my NP program. And crazy enough, I now work as a palliative care NP at Banner University Medical Center in Phoenix!
Thank you so much for putting into words how I have felt many times over the last few months. I absolutely love my job and work with an incredible team – but this COVID crap has been tough! I look forward to continuing to read your posts! I hope you and the family are staying safe and well.
Take care!
Cara
LikeLike
Thank you for this. I think the coroner who filled out my moms dc must have fallen into the lazy, didn’t care, didn’t know how column. He wrote 3 letters…not even the words. He probably didn’t know how to spell them. They were ALS. Yup.
LikeLike
I’m so sorry to hear about your mom. ALS is such a devastating disease.
LikeLike
Hey, Cuz! Great job … Now, two questions:
1. Can Covid kill without either pulmonary or cardiac effects?
2. Why would the CDC release this data, especially in the aftermath of the recent NYTimes article on too-sensitive Covid testing? Personally, I’d file that under “Not Helpful.”
LikeLike
Hi there! Hummm…I’m sure Covid could kill you without obvious pulmonary or cardiac dysfunction. The scenario I could come up with would be a massive stroke provoked by the hypercoagulable state that Covid can cause.
I suspect that the CDC was just publishing data that they had accumulated and didn’t anticipate that people would misconstrue it.
LikeLike
When it says “health conditions and contributing causes mentioned in conjunction with deaths involving coronavirus disease 2019 (COVID-19),” does that mean someone may have died of something else (I’m seeing covid deniers say this chart includes codes for assault, burns, and injury from car accident, for example) but also tested positive for Covid? It’s the one point I can’t (yet!) argue!
LikeLike
Great question! I went back and found instructions from our department of health and environment and this was the exact verbiage: “• COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death. Certifiers should include as much detail as possible based on their knowledge of the case, medical records, laboratory testing, etc. If the decedent had other chronic conditions such as COPD or asthma that may have also contributed, these conditions can be reported in Part II.” So covid should be listed if it contributed to or caused the death. It should not be listed if it was present, but didn’t contribute to death (ie. trauma).
LikeLike
Hey, great post and a really insightful response to the conspiracy theorists out there! Just a question on your terminology. Is it Sars-CoV-19? I’ve only ever heard of COVID-19, the disease caused by the virus SARS-CoV-2 which was previously known as 2019-nCoV. But maybe there are other terms I’m not aware of.
LikeLike
Michael! You are absolutely correct! In my rage, I totally missed that. It is SARS-CoV-2. Thank you for pointing that out. I will try to get that edited ASAP.
LikeLike
Should the presence of Covid-19 be reported somewhere else? I a retired pediatric UCU nurse and your explanations so impressed me and provided me with an abundance of information and knowledge. Thank you very much. I did not realize the true name of the virus. Thanks for that information too.
Having read a lot, although not a multitude, of posts on social media, I found your post well written with little if any editing needed!
LikeLiked by 1 person
THANK YOU!! Thank you for taking the time to explain all of that in depth and in terms everyone can understand, if they will just take the time to read it. I’m sharing this!
LikeLike
During a flu epidemic, do they routinely test every respiratory death to see if there are flu viruses present, or fragments of them?
Flu testing isn’t done at nearly the levels we test for COVID-19. In fact, most of the time local health agencies don’t even bother in many cases. Certainly nobody is running around testing healthy people to see if there’s virus or fragments in their systems. When I was looking at flu deaths in Santa Clara county in California, I found they simply didn’t take flu data at all for anyone 65 or older.
While that 6 percent may be artificially low, it seems obvious that authorities are working to push death statistics higher for COVID. That’s not even taking into account higher payments to hospitals for COVID-19 patients (true, but no hard evidence anybody is exploiting this fraudulently).
LikeLiked by 1 person
That’s an interesting question. Influenza is certainly tested for if a person presents to their doctor or hospital with symptoms, particularly if that information might guide their treatment (Tamiflu, etc). We generally wouldn’t “screen” for influenza the way we do for Covid because influenza isn’t as virulent as Covid. Sure the flu can spread and some people can get really sick and die (I’ve seen it first hand – get your flu shot!), but we’ve seen that Covid is capable of much worse, so it is more important to identify people with Covid to try to contain the spread as much as possible. Some preliminary numbers from the CDC on influenza statistics. 2018-2019 – estimated 35 million cases of influenza, 16 million medical visits, 490k hospitalizations and 34k deaths. I will be the first to point out that the data is not exact and is extrapolated from hospital visits, etc, because the proverbial “bang for your buck” just isn’t there to do widespread testing of influenza like it is for Covid (6 million cases in the US with 184k deaths).
LikeLiked by 1 person
You have provided hypothetical scenarios in your analysis to prove your point. One of them being a perfectly healthy 35 year old (how many real life examples can you point to where this has happened?). How is that helpful? It certainly isn’t scientific.
LikeLike
You are correct that the majority of those who die of Covid are not young and otherwise healthy. I was using that example to illustrate how a death certificate might be filled out in that scenario to explain why 3 different diagnoses might appear on that particular death certificate. I am obligated to respect patient privacy, therefore I cannot use anything other than hypothetical examples.
LikeLike
Thank you, Dr. Bartlett. I was referred to your blog here by my cousin who now lives in Valencia, Spain. Coincidentally, I had JUST finished reading an FB post regarding the CDC reporting of Covid at 94%. I’ve enjoyed reading your entire Covid posts here. Please don’t get too bored with them – please keep them coming. Thank you again! (fellow Kansan…Dodge City). Please stay safe.
LikeLike
So is it irrelevant that Medicare was/is paying huge bonuses for a single diagnosis of Covid19? …like $13-19,000 per single diagnosis. Na, I’m sure that didn’t influence any medical professionals while filling out these death certificates, ya think? Not to mention they also pay hospitals $39,000 if they put the patients on ventilators.
Comments?
LikeLike
Hi Dan! I have heard a lot of questions about this idea that hospitals are getting huge bonuses for covid patients. A few things. Billing and reimbursement are not tied to death certificates. Billing goes through the electronic medical record which is completely separate from the system that we use to complete and submit death certificates. Also, if someone is diagnosed with covid and ends up in the ICU on a ventilator for several days, 13k is not a “huge bonus” but rather a drop in the bucket in terms of the overall cost of that medical treatment. I just perused the CMS.gov website to try to learn more about this myself and there is additional reimbursement for Covid patients, but there has to be documentation of lab-confirmed Covid positivity to recoup this money (so an actual lab result confirming this, not just the doc says “covid positive.”). Another thing to consider is that Covid patients are more expensive to care for due to increased need for staffing, equipment, decontamination, extra PPE, etc. In terms of ventilators – early on there was anecdotal evidence (which was the best we had at the time) that early intubation lead to better outcomes. As the situation has evolved, that thought process has changed and our intensivists are finding that delaying intubation as long as possible and using things like non-invasive positive pressure ventilation and heated high flow oxygen lead to better outcomes. Additionally, intubation is a very high risk procedure for healthcare staff and so we really only do this when someone would otherwise die. When you insert and endotracheal tube through the mouth, throat and then into the airway, it causes a lot of respiratory droplets to be released into the environment (called and aerosolizing procedure). This puts the doc, RN and RT that are standing directly over the patient’s face during the procedure at increased risk of exposure and infection. So…another reason we only do this when it is absolutely necessary.
LikeLike
I am not a medical professional. It was a tough read for me. I can assure you the data is incorrect. My wheel house is the collection, transfer, storage and presentation of data. When we start talking probabilities or percentage of correctness we have left my wheel house. Of course the data is skewed towards the money. I don’t pay much attention to others opinions, I can get there myself. You must be extremely frustrated with whatever people are saying. I don’t know who the conspiracy theorists are or what they are saying and would like to. If you could provide a link I would appreciate it. Maybe I missed it. Anyway from my viewpoint, knowing little to nothing…I suspect people are dying at a higher rate than normal and covid probably has something to do with it. I was wearing a mask when the CDC, Surgeon General and Dr. Fauci told me not to. Glad to know they are now on board with my way of thinking. I believe, I got here logically, that masks protect the wearer as well as others. Apparently there is data to support that theory now, although it is still a theory scientifically speaking. I don’t need science to tell me barriers work. They keep things in and other things out. I leave the level of effectiveness to others. I do know space suits aren’t worn to protect space from us. I am looking forward to when medical science agrees with me on that. Perhaps more would wear masks if they thought it protected them. Anyway I digress. I am sorry you are so frustrated. You and others like you are superheroes. Logic gets me there also.
LikeLike
I’m neither a medical doctor nor a medical care professional. I am an attorney, and over the course of 4 decades, I advised and represented clients in cases involving death due to accidents or while in custodial care. As a result, I reviewed lots of autopsy reports and death certificates and consulted with medical experts about them. This article is an excellent explanation and confirmation of what I learned from that experience. I hope people will read this information, the BS all over the internet describing this data as supporting a conclusion that covid-19 caused deaths are grossly exaggerated is just plain wrong.
LikeLiked by 1 person
Hi Dr Bartlett – great explanations! Appreciate it. Trying to wrap my head around the underlying COD topic around this. As per the NCHS death certificate data, they currently list Covid as the underlying cause of death in 93% of the cases. Is this more an open interpretation that it was responsible as opposed to actually being listed as the underlying cause on the death certificate? I see from table 3 on the weekly report that there are plenty of diseases listed on the DC – cancer 7805, diabetes 27528, obesity 6059 etc – those make up quite a bit more than the other 7%. Wouldn’t these actually be the underlying though and covid the secondary COD/complication leading to primary COD? I understand the data well, but that part I can’t quite figure! Insight would be great!
LikeLike
As a clinical biochemist (med lab nerd), I am delighted to adopt your phrase, chronic rage, to finally describe my evolving mood over the last months. Thanks for this. Keep it up!
LikeLiked by 1 person
Hi! Melissa pharmacy head tech from Montreal, Canada. Thank you so so much for this explanation! It is really well appreciated!! 🙂
LikeLike
I understand your analysis, and that leads me to this question. Based on your description, even someone who dies of heart failure is likely to have more than one cause of death listed on the death certificate. But some way, some how, a certain number of deaths are reportedly “caused by heart failure” in a calendar year. Same for obesity and other health conditions. We then compare these statistics to conclude that, for example, one health condition is more deadly than another. What folks are trying to do is figure out how “deadly” is COVID19. If I have a lesser probability of being killed in a car accident on my way to work, or slipping and falling in the shower, then that informs me as to how much effort I should put into avoiding contracting COVID19. It’s one thing to spend $20 to buy a rubber mat for inside my bathtub. It’s another thing to shut down a trillion dollar economy completely. Based on your expertise, how do you suggest we determine how deadly COVID19 is, a new and unfamiliar cause of death, in context to some other causes of death, so that the general population has some way to understand it in relative terms to something with which we are familiar?
LikeLike